

Covid-19 e malattie cardiovascolari
Indipendentemente dalle infezioni di Covid 19, le malattie cardiovascolari sono ancora la causa più comune di morte in Svizzera. Sono responsabili di oltre 20.000 decessi nel nostro Paese ogni anno. Non esitate a chiamare il 144 in caso di sintomi, soprattutto di dolore al petto. Consultate la nostra pagina dedicata alle emergenze. Una diagnosi e un trattamento tardivi possono avere gravi conseguenze per la salute e il decorso della malattia.
Importance of Covid-19 in cardiovascular medicine
There is no question that cardiovascular medicine is influenced in various ways in Covid-19 disease [1,2]. The current state of research can be summarised as follows.
- COVID-19 diseases (COronaVIrus Disease 2019) are caused by the SARS-CoV-2 Virus (Severe Acute Respiratory Syndrome CoronaVirus 2), which was first observed in Wuhan (China) in 2019 [3] and has caused a worldwide pandemic [4]. SARS-CoV-2 belongs to the strain of the beta corona virus and is genetically 79.5% identical to the SARS-CoV virus[5] known since November 2002, which was also first observed in China (Foshan, Guangdong) and had also caused a worldwide pandemic in 2002/2003.
- Covid-19 can show severe disease progression. Studies show that 13.9% of cases are to be classified as "severe" and 4.7% as "critical". The roughly estimated case fatality rate for clinically recorded patients is 3.8% [6,7,8]. For the total number of all infected persons, more recent studies assume a much lower value. The lethality rate calculated by the John Hopkins University is 1.98% [4] and that of the so-called Heinsberg study is as high as 0.37% [9]. The lethality calculated by the Johns Hopkins University is 5 times higher than that of the Heinsberg study, which is explained by the different reference size of the infected persons. In the Heinsberg study, all infected persons are included in the sample, including those with asymptomatic and mild courses. In general, the values mentioned show strong country-specific variations, which is related, among other things, to different counting methods, high country-specific dark figures [10] and different compositions, especially demographic compositions, of the infected population strata [7,8].
- The risk of a severe or even critical course of the disease shows a clear age dependency [1,7,8,11-14]. Persons over the age of 65 are therefore classified by the Swiss federal government as particularly at risk.
- In addition, mortality is significantly higher in people with one or more previous illnesses, so-called comorbidities [1,7,8,11-14]. These include hypertension, diabetes, obesity and coronary heart disease [1,7,8,11-15]. Comorbidity is a further, diagnostically definable clinical picture that exists in addition to an underlying disease (index disease). However, for Covid-19, it is currently still unclear whether these diseases are only a marker for an increased risk of death or whether they actually influence the risk of death as mediators.
- Acute and fulminant myocarditis can occur in covid-19 disease [3,7,8,16-19]. These are usually associated with an unfavourable prognosis. Acute heart damage characterized by elevated troponin and/or electrocardiographic (ECG) or echocardiographic (cardiac ultrasound echo) changes has been observed in up to 17% of hospitalized COVID-19 patients.
- Cardiac troponin is a protein complex from the group of troponins. It is released from the muscle cells of the heart into the bloodstream in case of damage (e.g. heart attack). The maximum troponin level correlates with the survival rate after myocardial infarction. In addition, the level of troponin allows an estimation of the size of the infarction as measured by myocardial necrosis or damage to the heart. Of the troponins, troponin T and I are highly significant for cardiac events. They are the most important laboratory chemical parameter for Acute Coronary Syndrome (ACS). However, in the case of elevated troponin, other cardiac and non-cardiac diseases in addition to myocardial infarction also come into question as a possible diagnosis in the process of differential diagnosis.
- Until a vaccine has been developed, the most important thing for at-risk patients is the greatest possible active self-protection, so that these groups do not become infected in the first place. In this context, it is important to note that according to recent studies, up to 86% of all infected patients may show no symptoms (over 40%) or only such weak symptoms that they do not associate this with covid-19 disease [10,20]. These undocumented infected individuals contribute significantly to the spread of the virus and, as apparently healthy individuals, pose a particular risk to patients at risk if they do not protect themselves consistently[10,20].
Post-Covid-19 und Long-Covid-19
- Some patients experience persistence or onset of various symptoms associated with COVID-19 after recovering Covid-19 disease. This situation is referred to as post-covid-19 or long-covid-19. Patients with such ongoing symptoms after recovery from COVID-19 are increasingly recognized as a growing population in need of attention. By far, the most important causes of post-Covid-19 or long-Covid-19 symptoms include Covid-19-induced damage to the cardiovascular system and neuronal structures of the brain. Similar to other infections, especially influenza or Epstein-Barr virus diseases, these persistent symptoms extend beyond the resolution of the actual infection. Currently, a distinction is made between (i) long covid syndrome, when symptoms persist for more than four weeks, (ii) post covid syndrome, when symptoms persist for more than twelve weeks, and (iii) chronic covid syndrome, when symptoms persist for more than six months.
- A potential cardiovascular involvement can occur on multiple fronts, including:
- Myocardial (e.g., myocarditis)
- Pericardial (e.g., pericarditis)
- Myopericardial (e.g., myopericarditis)
- Coronary artery (e.g., microvascular dysfunction)
- Vascular (e.g., deep venous thrombosis, thrombophlebitis, pulmonary embolism)
- Published data indicate that as many as 60% of patients have evidence of active cardiac inflammation months after the original COVID-19 infection, and cardiac biomarkers, such as a detectable troponin level, have been seen in up to 71% of patients in the convalescent phase, regardless of severity and course of the acute illness.[21]
- At the Cardiovascular Center, patients with persistent symptoms following COVID-19 that may have an underlying cardiovascular etiology — such as chest pain, dyspnea, fatigue, heart palpitations or exertion intolerance more than four weeks after initial infection — undergo a focused evaluation to screen for cardiovascular complications. Patients who had COVID-19 can use the center whether or not they required hospitalization for their initial illness. In addition, patients with preexisting cardiovascular disease (e.g., hypertension, heart failure, atrial fibrillation) are evaluated who had COVID-19 of any severity in order to assess for possible changes in cardiovascular status. Patients are evaluated by the cardiologist and undergo ECG, echocardiography and laboratory tests, including cardiac biomarkers to assess cardiac function. Additional diagnostic tests — such as cardiac MRI, cardiac pulmonary exercise testing, patch rhythm monitoring, chest CT and lower extremity duplex testing — are offered according to individual symptoms and examination or test findings, in keeping with clinical standards. If required, p'atients are referred to subspecialists and resources from electrophysiology, sports cardiology, heart failure, cardiovascular imaging and vascular medicine, as indicated. After evaluation, patients are offered a personalized care plan, and cardiovascular treatments are started if appropriate. Patients will be followed until cardiovascular symptoms resolve.
- In any case, if you are among the risk or high-risk patients, e.g. in the case of high blood pressure or coronary comorbidities, do not hesitate to visit one of the test centers as early as possible and contact your doctor if there are signs of Covid-19 disease or if you had contact with infected persons.
Therapies with ACE inhibitor and Sartane
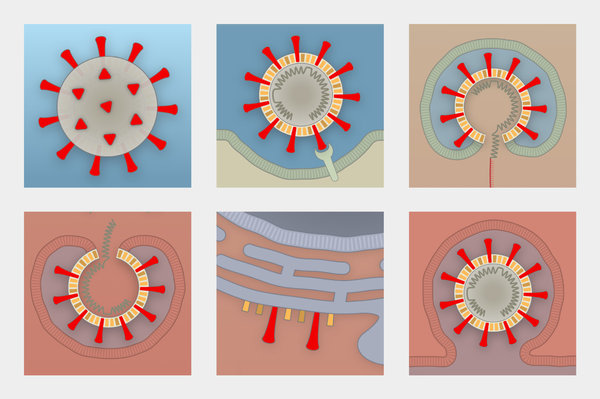
- The SARS-CoV-2 virus uses the receptor of the angiotensin converting enzyme 2 (ACE2) for cell entry. Moreover, studies have shown, at least in animals, that ACE inhibitors and Sartane increase the transcription of (cardiac) ACE2. This provides the basis for the much-discussed hypothesis that therapies with ACE inhibitors and Sartane and the overexpression of ACE2 could be associated with increased viral entry into the target cells and thus with a more severe course of COVID-19 disease [22-27].
- However, studies show that the SARS-CoV-2 virus also uses other receptors to enter the T cell, such as CD147, which is located on the surface of T lymphocytes [5]. For example, it has been shown that SARS-CoV-2 viruses can also infect T cells by receptor-dependent S-protein-mediated membrane fusion. These alternative pathways explain why certain studies suggest higher mortality when treated with ACE inhibitors or angiotensin receptor blockers, while other studies suggest that higher levels of ACE2 receptors may be protective.
- Larger clinical studies have not yet been able to prove a causal link between therapies with ACE inhibitors/artans and risks in covid-19 disease [26-28]. The reason for this seems to be that therapies with ACE inhibitors do not lead to higher ACE2 concentrations [26]. Conversely, the higher risk of disease in men compared to women [1,3,6,9,11-13] appears to be due to the higher levels of ACE2 in men's blood [29].
- The current consensus of medical societies is that these theoretical considerations should not influence therapy with ACE inhibitors or angiotensin receptor blockers if these drugs are clinically indicated.
Causes of death in Covid-19
- In covid-19 disease with a fatal outcome, patients typically develop sepsis associated with septic shock in over 60% of cases [3,8]. The most common actual causes of death are (i) respiratory arrest with acute lung failure, (ii) heart failure: In addition to the lungs, the heart is often severely affected by SARS-CoV-2. Severe acute damage, including heart failure, can occur. In case of a previous cardiovascular disease, the infection significantly increases the risk of death; and (iii) Cytokine Release Syndrome (CRS) with an overreaction of the immune system by hyperactive T-helper cells. The inflammatory wave can damage the intestine, liver, kidney, lungs, and particularly frequently the heart, up to cardiac arrest or respiratory arrest [29,30].
- The cytokine-release syndrome CRS, in its strongest form also known as cytokine storm or hypercytokinemia, is one of the most frequent causes of death in Covid-19 diseases, just as in SARS-CoV and MERS-CoV [21]. CRS is an overreaction of the immune system in which high concentrations of inflammation-relevant cytokines are produced, which in turn cause leukocytes to produce further cytokines (positive feedback). In CRS, high concentrations of the cytokines IL-6 and IL-8 and the chemokines CCL2, CCL5, CXCL10 and CXCL9 are produced.
- Particularly important in Covid-19 diseases is the IL-6 cytokine (interleukin-6), which belongs to the interleukins that regulate the body's inflammatory response. In beta-coronavirus infections of monocytes, macrophages and dendritic cells, this activates the production of Il-6 and other cytokines relevant to inflammation. Il-6 has a strong pro-inflammatory effect. The released cytokines are markers for the overreaction of the immune system (CRS) in Covid-19.
- Severe covid-19 disease with fatal outcome is therefore characterized by two critical phases of immune response. Firstly, an immune system underreaction or too slow an immune reaction, which leads to a high viral load in the nasopharyngeal area and subsequently to an infection of the upper and lower lung areas. In a second phase, an immune system overreaction follows, which can lead to cytokine release syndrome and may even lead to septic shock, cardiac arrest or lung failure.
SARS-CoV-2 infection routes and nasopharyngeal hygiene
- The routes of infection of SARS-CoV-2 viruses and the influenza viruses are comparable [31-33]. Like influenza viruses, the SARS-CoV-2 viruses pass from one carrier to the next by droplet infection when coughing, sneezing, speaking or shaking hands. Initially, the corona viruses multiply in the throat and nasal area, which are rich in cell surface receptors called angiotensin converting enzymes 2 (ACE2). If the immune response is insufficient, the viruses migrate from there, i.e. from the pharynx-nasal area, down the airways and infect first the upper lung areas and then the entire lung. Typical for Covid-19 disease is the bilateral infection of the lungs. In the upper airways (pharynx/nose), the route of infection is much shorter than when a pathogen first has to leave the lungs and enter the lungs of another person [31-33]. This explains the high rate of infection. SARS-CoV-2 viruses are also very virulent. This means that even small amounts of virus can trigger covid-19 disease [31-33].
- Studies show that the high viral load in the throat of Covid-19 right at the beginning of symptoms indicates that Covid-19 sufferers are infectious at a very early stage, often even before they even notice they are ill. At the same time, the infectivity of covid-19 patients seems to depend on the viral load in the throat or lungs [31-33].
- In addition, virus excretion is very high in the throat of COVID-19 patients, especially in adults, in the first week after the onset of symptoms. Large amounts of viral genetic material have also been detected in the cough sputum. Infectious virus particles could be isolated from both throat swabs and cough sputum. This means that the new coronavirus can multiply not only in the lungs but already in the throat and is therefore very easily transmitted [31-33].
- The risk of infection among risk groups in relation to other groups is not yet fully understood. However, at least one study seems to show that, in addition to an increased risk of severe covid-19 disease, risk groups often have a higher risk of infection [47], so double caution is needed for people in these groups.
- As the studies [31] suggest, we also recommend good nasopharyngeal hygiene for high-risk patients in particular, apart from the known precautions such as social distancing, wearing a mask and disinfecting hands [35,36], for the above-mentioned reasons in the event of possible contact with Covid-19 patients [34]. Gargling several times a day with a simple saline solution and cleaning the nasal passages with a saline solution-based rhinologue can help to reduce the virus load in the throat area and thus have a positive influence on a possible course of the disease. As a risk patient you should also try to live healthy, balanced and with enough exercise to positively influence your immune system. Avoid stress. Stress leads to the release of cordisol in the body, a body's own active cordisone. People with high cortisol levels have weaker immune defences because cordisol suppresses the immune response. Cortisol is also involved in the contraction of blood vessels in the body, thus increasing blood pressure. This can be particularly unfavourable for patients with already high blood pressure and can be stressful for the heart.
Covid-19 in children and cardiovascular risks
- Since the immune system of children can obviously control the virus load better, children, if they are infected at all, are often less infectious when they are sick. All available case numbers and studies seem to show that in children up to the age of about 15 years, smear-positive cases are rare with less than 1% of all those affected [37,38]. The causes may be lower expression of the receptor (docking site) for SARS-CoV-2 on respiratory cells and the absence of an exuberant immune response [39,40]. Furthermore, Covid-19 only shows a severe course of disease in a negligible percentage of children (e.g. in connection with the so-called Kawasaki syndrome [41-44]). In this sense, Covid-19 disease is a pediatric problem in very few cases. As far as is known so far, this also applies to children with cardiovascular disease as long as immune suppressants are not used for their treatment, e.g. in postoperative immune suppression after heart transplantation, or other disorders of the child's immune system are present.
- However, it is important to react quickly when there are signs of Kawasaki syndrome in young children [41-44]. Kawasaki syndrome (also known as Pediatric Multisystem Inflammatory Syndrome) is an inflammatory disease of the blood vessels (vasculitis). Kawasaki's syndrome is a leading cause of childhood acquired heart disease and vasculitis in young children. Kawasaki's syndrome is more common in infants and children, apparently associated with SARS-CoV-2 infection, and can cause irreversible damage to the arteries and veins that carry blood to and from the heart muscle (coronary arteries).
- For this reason, children and adolescents with high fever for several days and simultaneously high signs of inflammation (leukocytosis, high CRP) and an additional manifestation (exanthema, inflammation of the mucous membranes, gastrointestinal complaints, circulatory instability, etc.) should be referred to a pediatric clinic as soon as possible.
Scientific references and studies
- Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19; DOI: 10.1056/NEJMoa2007621, N Engl J Med (New England Journal of Medicine); May 01, 2020
- Coronaviruses and the cardiovascular system: acute and long-term implications; DOI: 10.1093/eurheartj/ehaa231, European Heart Journal; March 18, 2020
- Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study; The Lancet, Vol. 395, No. 10229; March 30, 2020
- Johns Hopkins University & Medicine: COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE); Covid-19 Case Tracker; Corona Resource Center at Johns Hopkins University & Medicine
- SARS-CoV-2 infects T lymphocytes through its spike protein-mediated membrane fusion; Nature, Cell Mol Immunol; April 07, 2020
- Estimates of the severity of coronavirus disease 2019: a model-based analysis; The Lancet, Vol. 395: 1054–62; March 09, 2020
- Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations; The Lancet, Vol. 395, Review, Published online; April 06 2020
- Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area; JAMA, DOI: 10.1001/jama.2020.6775, April 22, 2020
- Infection fatality rate of SARS-CoV-2 infection in a German community with a super-spreading event. (Heinsberg Study); University of Bonn (DE); Preprint Server, May 04, 2020
- Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2); Science 10.1126/science.abb3221; March 16, 2020
- Clinical features of patients infected with 2019 novel coronavirus in Wuhan; The Lancet, Vol. 395, No. 10223; February 15, 2020
- Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China; JAMA (Journal of the American Medical Association) Intern Med; March 13 2020
- Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019, February 12–March 28, 2020; MMWR Morb Mortal Wkly Rep 2020;69:382-386; March 31, 2020
- Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: a population-based cohort study; The Lancet, DOI: 10.1016/S0140-6736(20)30854-0; May 12 2020
- Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection?; The Lancet, Vol. 8, ISSUE 4, PE21; April 01 2020
- Potential Effects of Coronaviruses on the Cardiovascular System; JAMA Cardiology, Review March 27, 2020
- Cardiac Involvement in a Patient With Coronavirus Disease 2019 (COVID-19); JAMA Cardiology, Report March 27, 2020
- Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China; JAMA Cardiology, Published March 25, 2020
- Association of Coronavirus Disease 2019 (COVID-19) With Myocardial Injury and Mortality; JAMA Cardiology, Editorial March 25, 2020
- The natural history and transmission potential of asymptomatic SARS-CoV-2 infection; Clinical Infectious Diseases, Oxford University Press, DOI: 10.1093/cid/ciaa711, June 04, 2020
- Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19); JAMA Cardiology 2020;5(11):1265-1273; July 27, 2020
- Coronavirus Disease 2019 (COVID-19) Infection and Renin Angiotensin System Blockers; JAMA Cardiology, Published April 03, 2020
- The Dilemma of Coronavirus Disease 2019, Aging, and Cardiovascular Disease; JAMA Cardiology, Published April 03, 2020
- A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus–induced lung injury; Nature Medicine 11, 875–879; July 10, 2005
- Renin–Angiotensin–Aldosterone System Inhibitors and Risk of Covid-19; DOI: 10.1056/NEJMoa2008975, N Engl J Med; May 01, 2020
- Association of Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers With Testing Positive for Coronavirus Disease 2019 (COVID-19); DOI: 10.1001/jamacardio.2020.1855, JAMA Cardiol. Published online May 05, 2020
- SARS-CoV2: should inhibitors of the renin–angiotensin system be withdrawn in patients with COVID-19?; DOI: 10.1093/eurheartj/ehaa235, European Heart Journal; March 20, 2020
- Circulating plasma concentrations of angiotensin-converting enzyme 2 in men and women with heart failure and effects of renin–angiotensin–aldosterone inhibitors; DOI: 10.1093/eurheartj/ehaa373, European Heart Journal; May 10, 2020
- Cytokine release syndrome in severe COVID-19; Science 10.1126/science.abb8925; April 17, 2020
- COVID-19: consider cytokine storm syndromes and immunosuppression; The Lancet, Vol. 395, ISSUE 10229, P1033-1034; March 28, 2020
- Virological assessment of hospitalized patients with COVID-2019; Nature online; April 01, 2020
- Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study; The Lancet, Vol. 20, Published online; May 2020
- SARS-CoV-2 Reverse Genetics Reveals a VariableInfection Gradient in the Respiratory Tract; Cell 182, 1-18; DOI: 10.1016/j.cell.2020.05.042; July 23 2020
- Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional study; The Lancet, DOI: 10.1016/S1473-3099(20)30371-6; May 15, 2020
- Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1; DOI: 10.1056/NEJMc2004973, N Engl J Med; April 16, 2020
- Respiratory virus shedding in exhaled breath and efficacy of face masks; DOI: 10.1038/s41591-020-0843-2, Nat Med; April 03, 2020
- Children have a small role in the spread of COVID-19; National Institute for Public Health and the Environment, Nederlands; May 07, 2020
- COVID-19 in schools–the experience in NSW; National Centre for Immunisation Research and Surveillance (NCIRS), Australia; April 26, 2020
- Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults; JAMA, DOI: 10.1001/jama.2020.8707; May 20, 2020
- Nasal ACE2 Levels and COVID-19 in Children; JAMA, DOI: 10.1001/jama.2020.8946; May 20, 2020
- Hyperinflammatory shock in children during COVID-19 pandemic; The Lancet; DOI: 10.1016/S0140-6736(20)31094-1; May 07, 2020
- An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study; The Lancet; DOI: 10.1016/S0140-6736(20)31103-X; May 13, 2020
- Outbreak of Kawasaki disease in children during COVID-19 pandemic: a prospective observational study in Paris, France; medRxiv; DOI: 10.1101/2020.05.10.20097394; May 14, 2020
- Serum responses of children with Kawasaki Disease against SARS-CoV-2 proteins; medRxiv; DOI: 10.1101/2020.05.24.20111732; May 26, 2020
The origin of the SARS CoV-2 virus
- The proximal origin of SARS-CoV-2; Nature Medicine, Nat Med 26, 450–452; March 17, 2020
- Identifying SARS-CoV-2 relatedcoronaviruses in Malayan pangolins; Nature, Accelerated Article Preview Published; March 26, 2020